World Momentum Builds for Universal Health Coverage
World Momentum Builds for Universal Health Coverage

NEW YORK: It might seem surprising, but just as the world is recovering from the most serious financial shock since the World War II, governments around the world are engaging in serious discussions on how to expand health coverage.
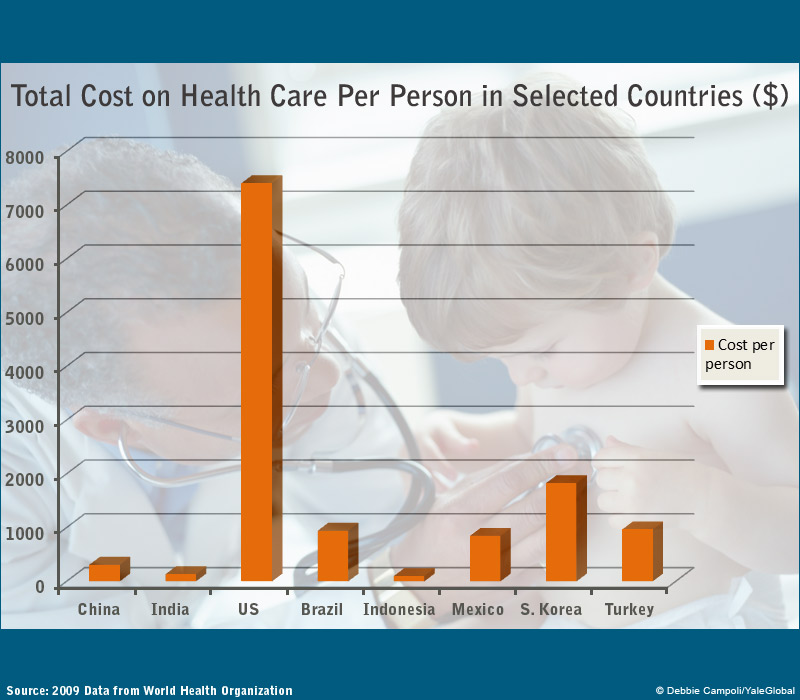
This new wave of universal health coverage, or UHC, has touched nearly 100 countries, all studying how to institute government-funded programs of health care. This concept is taking off in populous countries and traditionally UHC “blind spots,” such as Indonesia, China, India and South Africa. Combined, these four countries account for 40 percent of the world’s population. Unlike the US, emerging economies are not buying the argument that health care is largely the responsibility of individuals and businesses, with a public provision relegated to special interests, including the elderly, veterans and the indigent.
The first wave came in the 19th century after German Chancellor Otto von Bismarck introduced comprehensive medical care that covered large segments of blue-collar workers. Germany’s 1883 Health Insurance Bill and other social legislations formed the basis of the modern welfare state. In the post–World War era, most industrialized democracies and many socialist countries established health programs so that all people had access to affordable health care. According to the International Labor Organization, nearly 50 countries had attained near universal health coverage by 2008.
The next wave is among emerging economies.
In India, a national health-insurance scheme geared towards increasing access for the poor, known as RSBY, started rolling in April 2008. So far it has enabled 100 million to have cashless, paperless, portable access to inpatient health care provided by more than 8,000 public and private hospitals across the country. The country’s Planning Commission is considering a report from a high-level expert group, calling for provision of easily accessible and affordable health care to all Indians by 2022.
Similar dynamics are observed in China, which announced plans to pump $124 billion into its health sector in January 2009, in a bid to achieve “safe, effective, convenient and affordable” health care by 2020. By the end of 2011, 95 percent of the Chinese citizens have already been covered by some form of health insurance. While UHC programs and initiatives vary across countries, the government political and financial support allows the cost burden of health care to be shared widely and evenly, health care services to be better utilized, and the health status of individuals to steadily improve.
If all goes well, most of the world’s population will have access to affordable basic health care in one decade – a true milestone in human history in view of the fact that 1 billion people today lack access and 150 million people face catastrophic costs each year because of direct payments for health care.
It sounds counterintuitive that universal health care gains momentum as the global economy remains sluggish and many developing countries are still facing tight budget constraints. Financial capacity does matter.
The low-resource setting of many nations in sub-Saharan Africa may partially explain why only two countries, Rwanda and Ghana, have made significant strides toward UHC in this region. By contrast, robust economic development and fiscal revenue growth in China and India have enabled these governments to invest in their long-neglected health care sector.
That however does not mean that achievement of UHC is linked to a country’s GDP size. As noted by Laurie Garrett and others in a 2009 Lancet article, countries with low GDPs such as Costa Rica, Cuba, Gambia and Gabon attained more impressive prepaid coverage than countries with much higher GDPs. Indeed, countries that introduced nationwide health-insurance schemes are found not only in upper-middle and high-income economies, such as Brazil, Thailand and Taiwan, but also in low-income or lower-middle-income economies, including Bangladesh, Philippines and Sri Lanka.
Many of these economies, including Sri Lanka, Malaysia and Indonesia, and to a lesser extent, Brazil and Thailand, have adopted some key aspects of the Beveridge Model which funds UHC through a government service paid directly through tax revenue. Others, such as Taiwan, Mexico and Turkey, choose the national health insurance model under which payment comes from a government-run insurance program that covers every citizen. Still others, such as South Korea and Costa Rica, rely on compulsory social health insurance financed jointly by employers and employees through payroll reduction, or the Bismarck Model.
In most countries, though, UHC is pursued through a mixed model of funding. Chile, for example, finances UHC through a public social insurance fund that combines the Bismarck contribution model with tax-financed care under the Beveridge approach for those without income.
Political commitment and health-system capacity are equally critical in this process. According to Kwesi Eghan, a senior program associate for the nonprofit international health organization Management Sciences for Health, many African governments lack the political will to introduce UHC plans or the ability to develop innovative funding mechanisms to pay for them.
Despite decades of robust economic growth, China and India did not seriously consider UHC until it became clear that economic development does not trickle down. For China, the fourth-generation leaders’ populist lurch coupled with the 2002-03 SARS debacle and the 2008 global financial crisis underscored the need to expand health care to stimulate domestic consumption and ensure social-political stability. For India, the government pays more attention to UHC than before not only because it’s convinced of the necessity of a healthy labor force to compete in the global economy, but also because the delivery of public goods and services has become an election issue since the mid-2000s. As former vice president of the World Bank, David de Ferranti, recently noted, in implementing UHC it is often 90 percent about the politics and 10 percent technical design.
Of course, at issue is not just scalability, but sustainability as well. How to sustain existing programs instituted for achieving UHC is a major concern in low-income and lower-middle-income economies. In Rwanda, a nation with a successful UHC program, foreign donors contributed 53 percent of the country’s total health expenditure. In Sri Lanka, another successful example, there is concern about the government’s ability to continue to provide health services free at the point of delivery.
Indeed, UHC programs in even high-income economies are struggling to cope with rising health-care costs, flattening economic growth, the globalization of diseases, population aging, the rise of non-communicable diseases and increasingly costly medical technology.
The foremost challenge however is to ensure that money is spent on targeted beneficiaries, which would entail improving efficiency and quality on the supply side. As William Hsiao of Harvard University observed, in almost all the countries implementing national health insurance, most of the money spent ultimately went into the pockets of doctors, nurses and other hospital staff. Again, political commitment is needed to reform the system to avoid UHC becoming another income-transfer program.
More than three decades ago, French philosopher and social theorist Michel Foucault reminded us that the principle aim of political rule was to “improve the condition of the population, to increase its wealth, its longevity, and its health.”
Population health and well-being are issues of governance. No matter how imperfect many existing UHC schemes may be, they constitute a global movement worth sustaining.
Comments
I commend the author for this article for the population's knowledge and clarity of the subject matter.
I'm sorry that without searching for this research topic it is not available on the first page of any Google Search.
An informed public is imperative given the 2020 primary elections.
For me and my children, whom I am exposing to multi opinions and fact-based information I thank you.
Travis Bodine; father, husband, veteran, and grandfather